


This guide is for Australian RTOs — trainers, assessors, student support officers, compliance managers, and leaders.
It draws on the DEWR VET student mental health and wellbeing resources (January 2026), Standards for RTOs 2025, Disability Discrimination Act 1992 (DDA), Disability Standards for Education 2005 (DSE), and best-practice frameworks from headspace, Beyond Blue, and ADCET.
Note: This resource does not constitute clinical or legal advice. Refer students to qualified professionals for diagnosis and treatment.
Australia’s VET sector enrols approximately 4.2 million students each year. Many arrive carrying pressures that go well beyond their course requirements: financial stress, housing insecurity, family responsibilities, cultural adjustment, past trauma, and undiagnosed or undisclosed mental health conditions.
Research consistently shows that young adults aged 16-24 — a significant proportion of VET enrolments — experience elevated rates of anxiety, depression, and psychological distress. For international students on CRICOS-registered programs, these challenges are compounded by language barriers, separation from family, and the pressure of maintaining attendance and course progress to satisfy visa conditions.
Under the Standards for RTOs 2025, RTOs have explicit obligations to support the wellbeing and progression of every student. The Disability Discrimination Act 1992 and Disability Standards for Education 2005 reinforce that mental health conditions are a form of disability requiring proactive, needs-based support — not just reactive crisis management.
The shift the DEWR guidance models is important: move away from the medical model (diagnosis-first, deficit-focused) toward a needs-based model. You do not need a student to hand you a psychiatrist’s letter before you offer support. If a student’s participation or progress is being affected by something — visible or not — your duty to respond begins.
Why This Matters for Your RTO
Mental health challenges rarely announce themselves with a formal disclosure. More often, they show up as subtle changes in behaviour, engagement, or presentation. RTO staff who interact with students regularly are in a powerful position to notice when something has shifted — if they know what to look for.
Watch for changes from a student’s established pattern:
The Concept of Imputed Disability (DEWR Guidance)
You do not need a formal diagnosis to act. The DEWR guidance materials and DDA 1992 recognise ‘imputed disability’ — where an RTO has reasonable grounds to believe a student’s participation is being affected by a mental health condition, even if no diagnosis has been disclosed.
If you see the signs, you have a responsibility to reach out. Waiting for a student to self-identify before offering support is not sufficient.
One of the biggest barriers to student support is not the absence of resources — it’s the discomfort staff feel about initiating a conversation about mental health. Most trainers and assessors are not counsellors, and they shouldn’t try to be. But they can listen, express genuine care, and connect students to the right people.
The DEWR guidance materials emphasise that effective student support begins with the quality of the conversation, not the complexity of the system behind it. A single well-handled conversation can be the turning point for a student who is struggling in silence.
The R U OK? The model provides a practical four-step structure that any staff member can use:

| SAY THIS | AVOID THIS |
|---|---|
| “I’ve noticed you seem to be having a tough time — would you like to talk about it?” | “What’s wrong with you lately?” |
| “You don’t have to share anything you’re not comfortable with.” | “You just need to push through it.” |
| “I’m not here to judge — I just want to make sure you’re OK.” | “Everyone feels like that sometimes.” |
| “There are people here who can help — would you like me to connect you?” | “Have you tried just focusing more in class?” |
| “Would it help to take a short break from your assessments while we sort out some support?” | “You need to see a doctor before we can do anything.” |
| “Your progress here matters to us — and so do you as a person.” | “I’m not trained to deal with this.” |
When a student discloses a mental health concern, do the following:
Confidentiality and Its Limits
Students should understand that their disclosure is treated with respect and discretion, but it is not unconditional confidentiality. If a student discloses that they or someone else is at risk of harm, you have a duty of care that overrides confidentiality.
Tell students this at the start of sensitive conversations: ‘What you share with me stays within our support team unless I believe someone is in danger — in which case, I’d need to get you further help.’
Internal support does not require a clinical team. It requires a clear process, trained staff, appropriate documentation, and a culture that treats student wellbeing as core business — not an afterthought.
Once a student’s need has been identified, develop a Student Support Plan in collaboration with the student. The DEWR toolkit provides ready-to-use templates. A good plan includes:
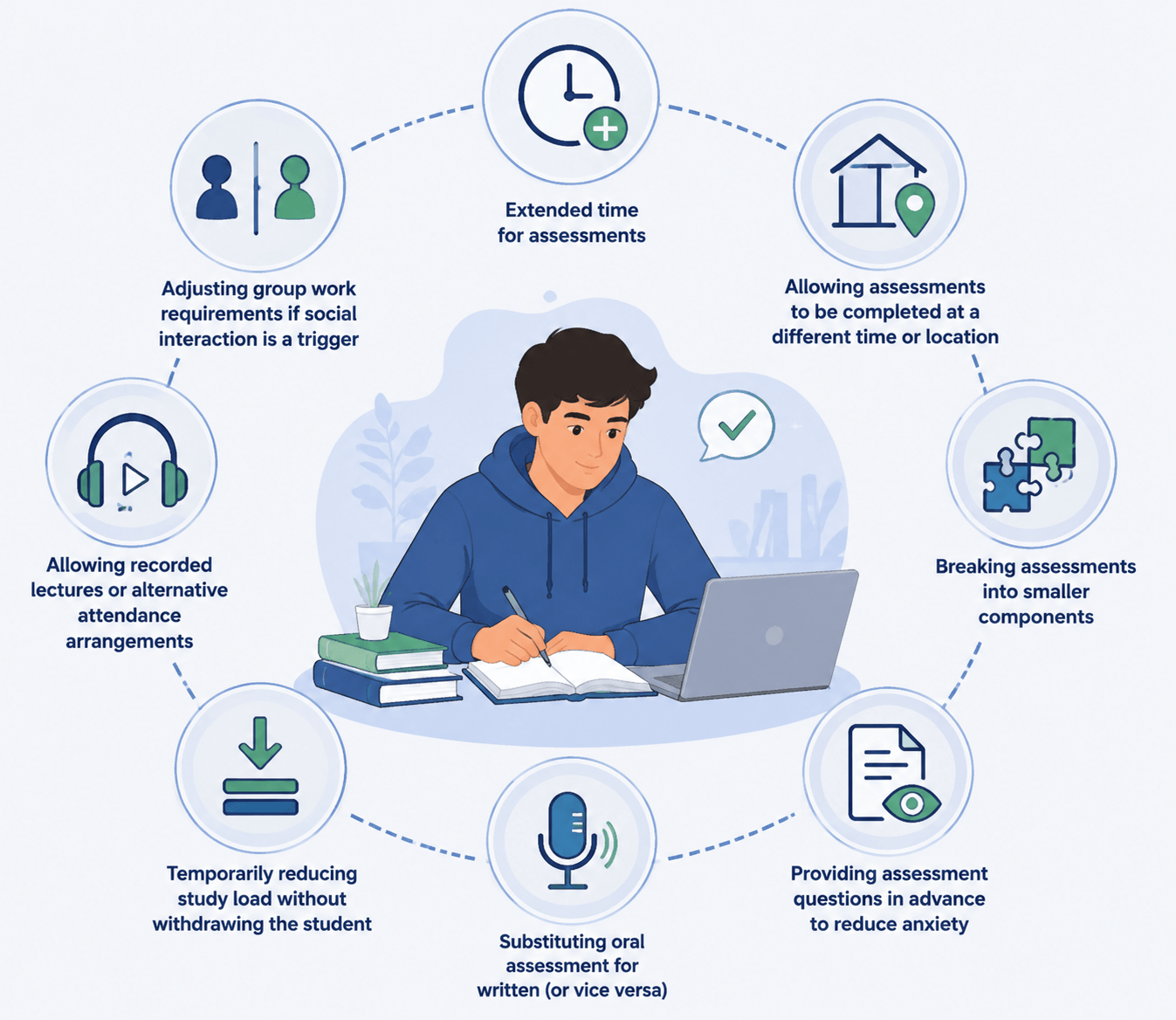
Reasonable adjustments must not compromise the core competency requirements of a unit but can include:
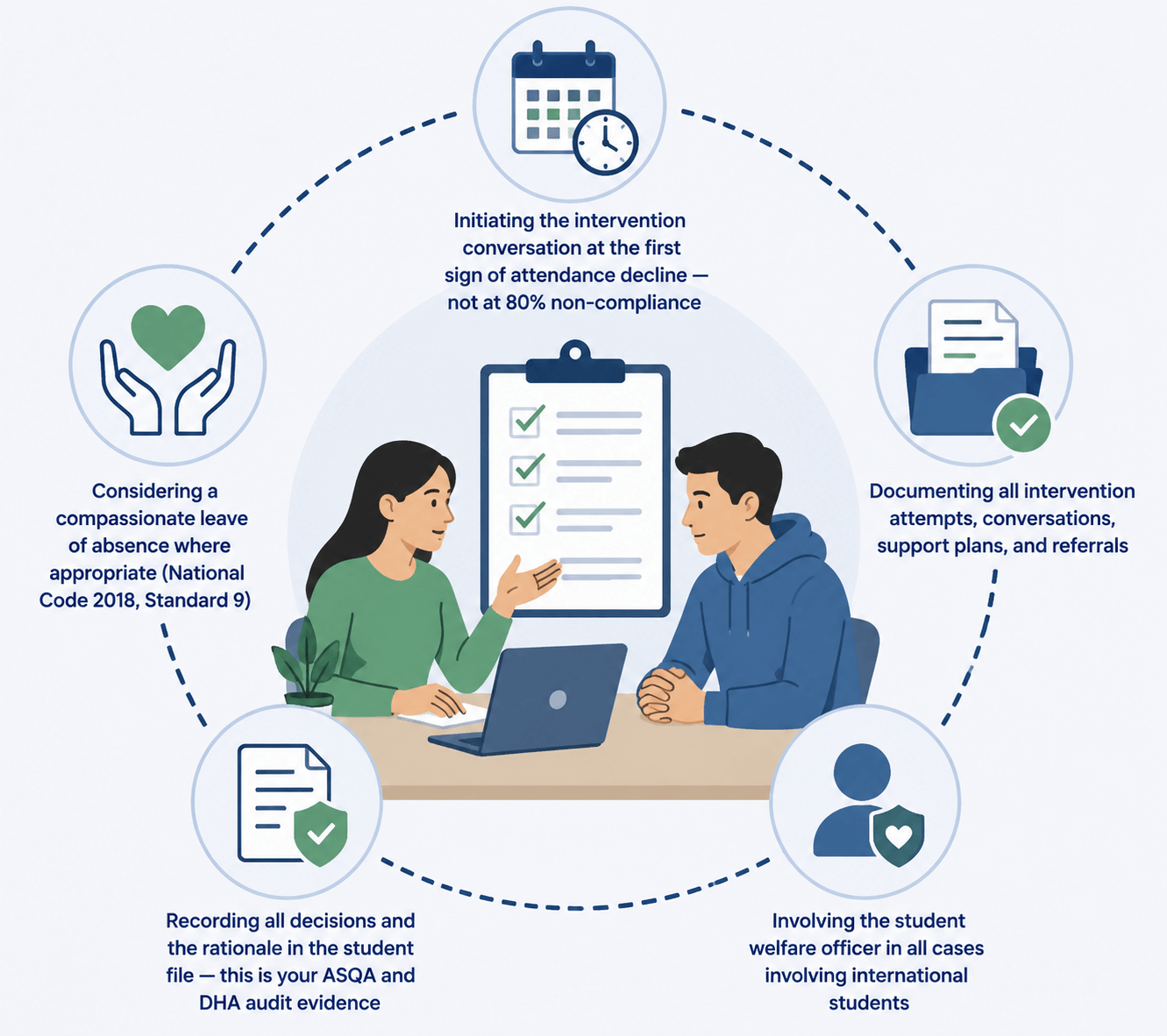
For international students on student visas, attendance and satisfactory course progress are conditions of visa compliance. A student struggling with mental health may begin missing class and falling behind, which triggers reporting obligations under PRISMS.
The correct approach is not to ignore the compliance trigger but to document the intervention before it reaches the reporting threshold. This means:
Universal Design for Learning (UDL) — Build It In, Don’t Bolt It On
The DEWR guidance strongly promotes Universal Design for Learning — designing training and assessment from the outset to accommodate diverse needs.
When accessibility is built into delivery rather than retrofitted via individual adjustments, it benefits all students and reduces the administrative burden on RTOs.
Practical examples: Providing learning materials in multiple formats, building regular check-in moments into lessons, creating low-stakes formative tasks alongside high-stakes assessments, and normalising the option to speak with a support officer.
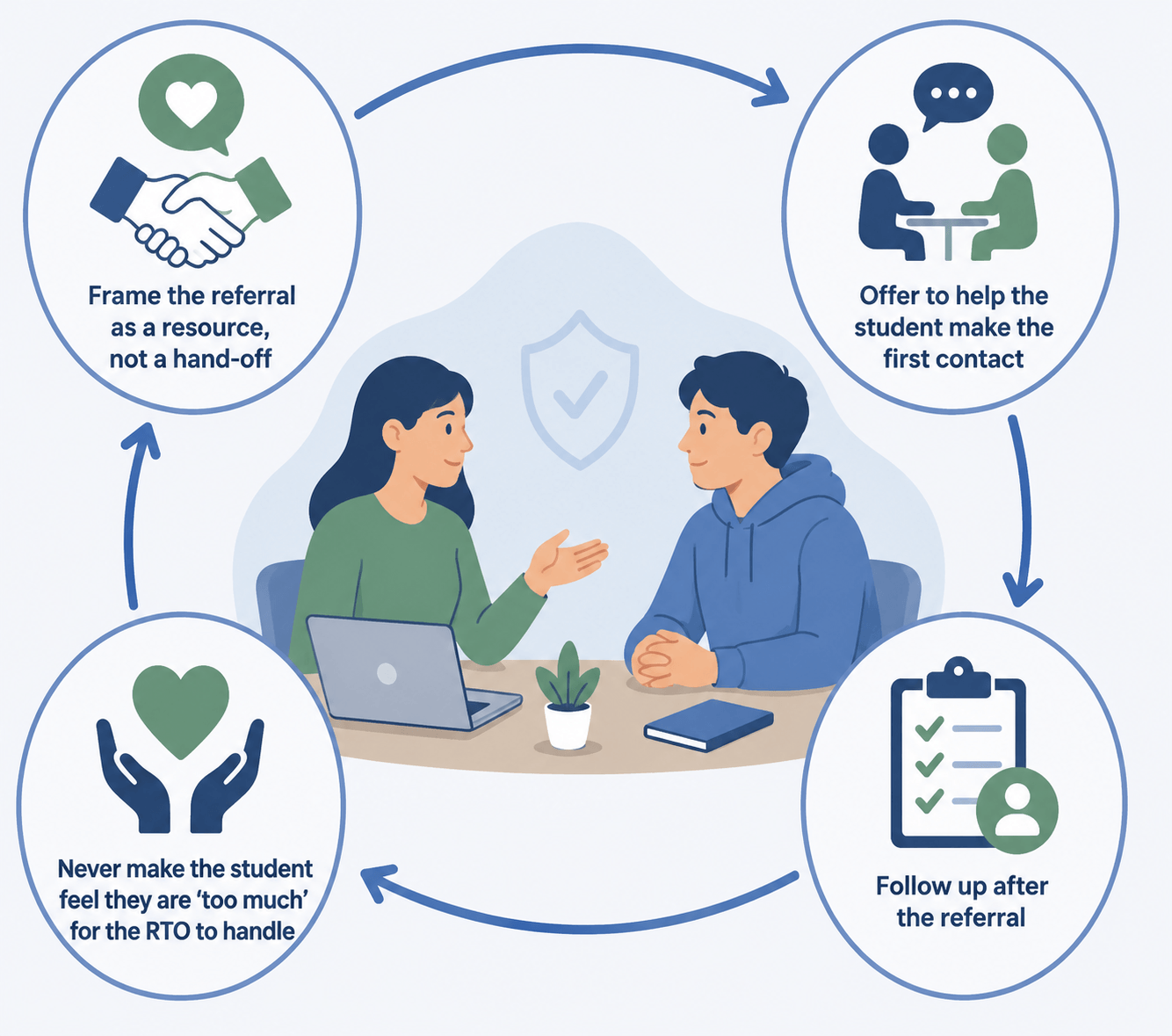
Internal support has its limits. Trainers and assessors are not counsellors, and they should not attempt to fill that role. Part of providing genuine support is knowing when and how to refer — and making that referral feel like an act of care, not dismissal.
| Organisation / Service | Phone | Website |
|---|---|---|
| Lifeline (24/7 Crisis) | 13 11 14 | lifeline.org.au |
| Beyond Blue | 1300 22 4636 | beyondblue.org.au |
| headspace (12-25 yrs) | 1800 650 890 | headspace.org.au |
| Head to Health | 1800 595 212 | headtohealth.gov.au |
| Suicide Call Back Service | 1300 659 467 | suicidecallbackservice.org.au |
| 13YARN (First Nations) | 13 92 76 | 13yarn.org.au |
| MensLine Australia | 1300 78 99 78 | mensline.org.au |
| QLife (LGBTIQ+) | 1800 184 527 | qlife.org.au |
| 1800RESPECT (DFV) | 1800 737 732 | 1800respect.org.au |
| SANE Australia | 1800 187 263 | sane.org |
| Black Dog Institute | blackdoginstitute.org.au | |
| ADCET | adcet.edu.au | |
| DEWR VET Wellbeing Resources | dewr.gov.au |
Emergency Protocol
If a student is in immediate danger or expressing active suicidal intent:
All RTOs should have a Critical Incident Policy and at least one staff member trained in Mental Health First Aid.
Good support and good compliance are not in tension. Documenting student support conversations, plans, and referrals protects the student, protects your staff, and protects your RTO at audit. Under the Standards for RTOs 2025, ASQA expects RTOs to demonstrate — not just claim — that they have supported students to the required standard.
The DEWR toolkit includes both an RTO Self-Check and a Trainer and Assessor Self-Check, rated on a three-level scale: Beginning, Developing, and Competent. Running your team through these tools annually will:
The following case studies are based on scenarios that occur commonly in RTO settings. All names and identifying details are fictional. They are intended for staff training and discussion purposes.
Mei, a 21-year-old domestic student enrolled in Certificate III in Individual Support, began submitting assessments late, then stopped altogether. She had been a strong student in Term 1. Her trainer noticed she was sitting at the back, not interacting, and had stopped eating lunch with her usual group.
The trainer waited until after class and asked Mei privately if she was doing OK. Mei disclosed she was experiencing severe anxiety about failing and had stopped sleeping properly. The trainer acknowledged her courage, assured her the conversation was confidential within the support team, and walked her to the student support office that afternoon. A Student Support Plan was developed, assessment deadlines were extended by two weeks, and Mei was referred to headspace.
Mei resumed assessments within three weeks and completed the qualification on time, rolling one unit into the following term. The RTO documented all intervention steps, providing a clear evidence trail. Mei later provided a written thank you to the support officer.
Ahmed, a 24-year-old international student enrolled in Diploma of Business (CRICOS-registered), began missing Monday morning classes. By week six, his attendance had dropped to 72%. His trainer raised a concern flag via the LMS. Ahmed had not responded to two emails.
The student welfare officer called Ahmed and arranged a face-to-face meeting. Ahmed disclosed he had been experiencing low mood since arriving in Australia, was struggling to make friends, and felt unable to tell his family he was not coping. The welfare officer acknowledged his experience and explained that attendance was approaching the reporting threshold — but that the RTO’s first goal was to support him, not report him. A modified attendance arrangement was developed for four weeks, along with weekly check-ins and referral to a free community counselling service.
Ahmed’s attendance recovered to above 80% by week ten. He did not trigger a formal PRISMS non-compliance event. The RTO maintained comprehensive documentation of all intervention steps. Ahmed later requested to extend enrolment by one term due to delayed progress, which was approved with appropriate supporting documentation.
During a one-on-one assessment feedback session, a 19-year-old student named Jordan said off-hand: “Sometimes I think about just not being here anymore.” The assessor paused, unsure how to respond.
The assessor calmly and directly asked: “That’s something I want to make sure I understand — are you having thoughts about ending your life?” Jordan confirmed they had such thoughts but had not made a plan. The assessor did not leave Jordan alone. They called the student support manager, who attended within minutes. The assessment was set aside. The support manager contacted Lifeline with Jordan present and helped Jordan speak to a crisis counsellor. Jordan’s emergency contact was called (with consent). The incident was documented as a Critical Incident per the RTO’s policy.
Jordan took a two-week leave of absence. On return, a comprehensive Student Support Plan was implemented including welfare check-ins, assessment adjustments, and referral to a local mental health service. Jordan completed the qualification in the following intake. The RTO’s prompt and documented response was noted positively in a subsequent ASQA desktop audit.
Tom, a 17-year-old enrolled in Certificate II in Construction, was increasingly disruptive in class — unable to sit still, frequently derailing conversations, and struggling to complete written tasks. His trainer assumed behavioural issues. After a warning letter was drafted, a more senior staff member suggested a different approach.
Rather than proceeding with the warning, the student support officer met with Tom and his parent. Using open questions, the officer discovered Tom had never been assessed for a learning disability or ADHD and had left school early partly due to these struggles. The RTO applied the concept of imputed disability and developed support measures without waiting for a formal diagnosis: flexible seating, shorter written tasks supplemented with oral responses, and a referral to a GP for assessment.
Tom’s participation improved significantly within four weeks. He later received an ADHD diagnosis and obtained formal reasonable adjustment documentation. He completed the certificate and expressed interest in continuing to Certificate III. The RTO’s proactive, needs-based approach was compliant with both the DDA 1992 and the Standards for RTOs 2025.
No. The DDA 1992 and DEWR guidance recognise ‘imputed disability’ — if you reasonably believe a student’s participation is being affected by a mental health condition, you are required to offer appropriate support regardless of whether a diagnosis exists. Requiring documentation before acting is both poor practice and potentially discriminatory.
No. You cannot compel a student to accept support. However, you must document that support was offered, how it was communicated, and the student’s response. If attendance or progress subsequently deteriorates to a compliance threshold, your documented offer of support demonstrates the RTO’s good faith. Keep the door open — follow up periodically.
At a minimum: a written Student Support Policy that references mental health; at least one staff member with a Mental Health First Aid certification; a list of external crisis and support resources provided to every student at enrolment; a clear process for how a student can request support; and a mechanism for staff to escalate concerns. The DEWR toolkit templates are free and can be adapted immediately.
The two are not mutually exclusive. Under the National Code 2018 and ESOS Act, intervening early and documenting the process is the correct approach. A compassionate leave of absence or modified attendance arrangement, properly documented, demonstrates that the RTO acted appropriately. The risk is not in showing compassion — it’s in ignoring the issue until the reporting threshold is reached without any documented intervention.
Take it seriously — every time. Ask directly if they are thinking about ending their life (this does not plant ideas). Do not leave them alone if you believe they are at immediate risk. Call 000 if there is immediate danger. Contact Lifeline (13 11 14) or Beyond Blue (1300 22 4636) for guidance in a crisis. Document the incident as a Critical Incident and follow your RTO’s Critical Incident Policy. Notify management immediately.
Absolutely not. Trainers are expected to notice, ask with care, listen without judgement, and connect students to the right support. The clinical work belongs to qualified professionals. The RTO’s role is to build the bridge between the student and those professionals — and to create conditions where students feel safe enough to cross it.
Yes, if there is a risk to the student’s or another person’s life or safety. Inform students at the outset of sensitive conversations that confidentiality has limits. When you do need to act on a disclosure that involves risk, tell the student what you are doing and why — transparency preserves trust even when confidentiality must be limited.
Under the Standards for RTOs 2025, ASQA expects RTOs to demonstrate that students are genuinely supported to participate and progress. Documented student support plans, referral records, and follow-up contacts are direct evidence. The DEWR self-assessment tools (RTO Self-Check and Trainer Self-Check) generate additional evidence of continuous improvement. Proactive mental health support practice reduces ASQA risk — it does not increase it.
Mental health support in VET is not a separate function from quality training delivery — it is integral to it. A student who is struggling with their mental health cannot learn effectively, cannot perform authentically in assessments, and cannot transition successfully into the workforce.
The DEWR guidance materials released in January 2026 give every Australian RTO — regardless of size or sector — the tools to do this well. The templates, practice guides, self-assessment instruments, and practice illustrations are freely available. There is no longer a resource gap; there is only an implementation decision.
At the heart of all of this is something that cannot be downloaded: a culture of genuine care. That culture is built one conversation at a time, by trainers who notice, assessors who ask, and support staff who follow through.


